

What is Ebola and why is stopping the latest outbreak so difficult?
Getty Images
An Ebola outbreak in the Democratic Republic of Congo has been declared a public health emergency of international concern, by the World Health Organization (WHO).
The latest outbreak is challenging because it involves a rare species of Ebola for which there is no vaccine, and the epicentre is in an area affected by conflict.
What is Ebola and what are the symptoms?
Ebola is a rare but deadly disease caused by a virus.
Ebola viruses normally infect animals, typically fruit bats, but outbreaks among humans can sometimes start when people eat or handle infected animals.
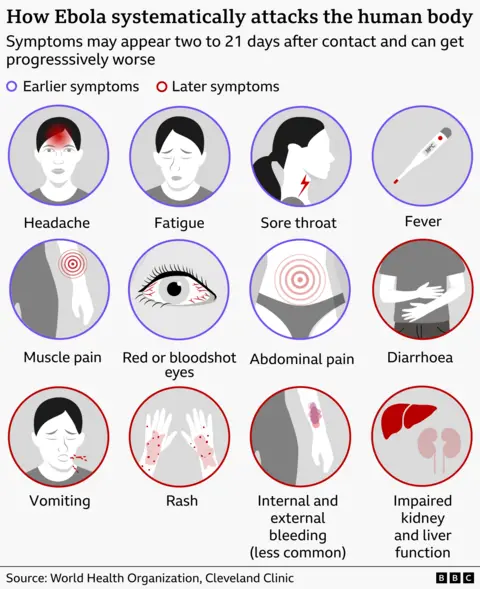
It takes two to 21 days for symptoms to appear. They come on suddenly and start like the flu or malaria, with fever, headache and tiredness.
As the disease progresses, vomiting and diarrhoea develop and it can lead to organ failure. Some, but not all, patients develop internal and external bleeding.
The virus spreads from one person to another by contact with infected bodily fluids such as blood or vomit.
Ebola outbreaks used to be small and contained to remote rural areas. However, urbanisation is pushing larger populations closer to these natural reservoirs of Ebola and increasing the risk of transmission.
Why is this Ebola outbreak different and is there a vaccine?
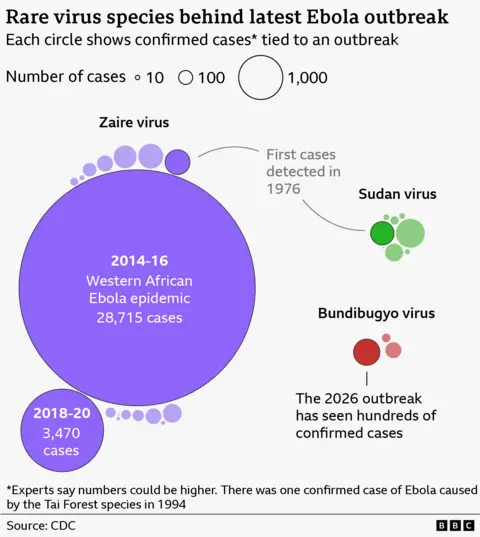
This outbreak is caused by the rare Bundibugyo species of Ebola, which had not been seen for over a decade.
Named after a district in Uganda where it was first detected, Bundibugyo has only caused two previous outbreaks – in 2007 and 2012.
One study showed that it killed about a third of those infected, far less than the more common Zaire (66.6%) and Sudan (48.5%) species. About 28% of those known to have been infected in the current outbreak have died.
Initial blood tests for Ebola in the affected areas were negative as they were designed to identify the more common form of the disease.
In July, the UK’s medicines regulator, the MHRA, said it had given permission for the first human trials of a vaccine for Bundibugyo to go ahead.
It was created by a team from the University of Oxford based on the same technology used in the Oxford-AstraZeneca Covid vaccine.
It took scientists just eight weeks to develop the new jab after plugging in genetic code from the Bundibugyo species of Ebola.
It will now be tested on 50 volunteers from Oxford aged 18 to 55 to see whether it triggers the correct antibody response without causing significant side effects.
Three other groups are also developing different vaccines for Bundibugyo although they have not yet entered clinical trials.
While treatments are available for other species of the Ebola virus, no drugs have been specifically approved to treat those infected with Bundibugyo.
The WHO is sponsoring a separate clinical trial in the DRC to see whether two existing antiviral therapies can improve survival rates.
The two drugs selected as the most promising are an experimental monoclonal antibody called MBP134 and remdesivir, an injection into a vein, which is also used to treat Covid.
A further complication is that the outbreak is taking place in a conflict zone, with a quarter of million people displaced from their homes and people moving across porous bordersinto neighbouring countries.
Trish Newport, from medical charity Doctors Without Borders, who is heavily involved in efforts to tackle the outbreak, told the BBC World Service that territory constantly changed hands between different armed groups, making it difficult for emergency response teams to simply drive to Ebola hot-spots.
She pointed out that a further problem was bad roads, with a 90km (56-mile) journey from Bunia city to Mongbwalu, one of two gold-mining towns where the majority of cases have been reported, taking more than three hours.
However, the WHO’s declaration of a public health emergency of international concern does not mean we are in the early stages of a Covid-style pandemic. The risk Ebola poses outside Central and East Africa is minimal.
How did the current Ebola outbreak start?
The first known case was a nurse who developed symptoms on 24 April, which means the virus had been spreading undetected for weeks.
The nurse died in Bunia, the capital of eastern DR Congo’s Ituri province, according to Congolese Health Minister Samuel Roger Kamba.
The victim’s body was repatriated to Mongbwalu.
Kamba said one of the reasons the virus spread so quickly was the number of people exposed to the body during the funeral ceremony.
Africa’s public health agency, the Africa Centres for Disease Control and Prevention (Africa CDC), told the BBC World Service that funerals were a particular concern, as they also helped spread the disease during previous outbreaks.
Africa CDCdirector Dr Jean Kaseya said public health information campaigns were “providing information on how to handle funerals” and the importance of basic hygiene and sanitation, as well as providing protection measures for health workers.
Kamba said there had been delays in reporting Ebola cases because infected communities believed the disease to be “witchcraft” or a “mystical illness”, resulting in people seeking treatment from prayer centres and witchdoctors rather than hospitals.
How many Ebola cases have been reported and where are they?

WHO chief Tedros Adhanom Ghebreyesus said he was “deeply concerned about the scale and speed of the epidemic”.
On 12 July, official said there had been 1,792 confirmed cases and 625 confirmed deaths from the virus in DR Congo.
There have also been 189 recoveries from Ebola so far, including four nurses whose discharge from hospital was celebrated at a special ceremony.
Ituri province is the epicentre of this outbreak and accounts for the vast majority of confirmed infections.
Officials in neighbouring Uganda have so far confirmed two deaths from Ebola – individuals who had travelled to Uganda from DR Congo. The authorities there have also confirmed 20 cases, with 15 people recovering from the virus.
France confirmed its first case on 24 June – a doctor who had returned from a humanitarian mission in the DR Congo.
In early June, he was discharged from a hospital in Germany, where had been evacuated to for treatment.
Cases have also been confirmed in North Kivu (44) and South Kivu (3), provinces partly controlled by the rebel AFC-M23 alliance. These discoveries signalled the outbreak’s spread from its epicentre.
What is being done in DR Congo to tackle the current Ebola outbreak?

Getty Images
Mass gatherings have been banned in the provinces with confirmed cases – Ituri, North Kivu and South Kivu – as well as three neighbouring provinces – Tshopo, Haut-Uele and Bas-Uele.
Capital city Kinshasa – which has no confirmed cases and is located some 1,800 km (1,100) miles from the outbreak – has also been ordered to ban mass gatherings. The French doctor had travelled through the city on his way home.
The Congolese government has established four laboratories in Ituri – in Bunia, Mongbwalu, Beni and Aru – which can test blood samples for the Bundibugyo species of Ebola. Results can now be delivered within 24 hours, removing earlier delays.
Surveillance systems, contact tracing and the treatment infrastructure, with dedicated centres in several affected towns, have also been expanded, according to the health minister.
The WHO has dedicated $3.9m (£2.9m) to tackling the outbreak, while Africa CDC has announced a $319m budget. South African President Cyril Ramaphosa has pledged an initial $5m to support the agency’s plan.
A toll-free number, 151, has been provided for reporting symptoms and people are being reminded to:
- avoid contact with bodies of people who died with symptoms, or with dead animals
- not eat raw meat, as undercooked food may transmit the virus
- practise social distancing.
How have the rebels responded to the latest Ebola outbreak?
The AFC-M23 group has created an Ebola response team in an effort to prevent transmissions in the areas it controls.
Spokesman Lawrence Kanyuka said the group was working with health services and local medical facilities.
Neither the government nor the rebels have explicitly said whether they are prepared to work together to tackle the outbreak.
However, a case in Goma, North Kivu’s provincial capital, was confirmed by a state-run body, the INRB.
Caitlin Brady, the country director for the Danish Refugee Council, said that earlier on in the outbreak, the M23 told her they were using contact tracing and all appropriate measures to contain the virus.
“A lot of the health officials and healthcare workers stayed and continued working” after rebels seized the city, meaning “the capacity to respond has remained”, Brady told the BBC World Service’s Newsday programme.
What are Rwanda and other neighbouring countries doing about the Ebola outbreak?
Rwanda closed its borders with DR Congo earlier on in the outbreak. According to Congolese media, authorities began to reopen parts of the border late in June following a lull in local infections.
Uganda has temporarily suspended flights, buses and all other public transport crossing the border with DR Congo.
After the first cases were detected in Uganda, authorities there told people to avoid hugging and shaking hands.
Several other African countries are tightening border screenings and bolstering health facilities.

Getty Images/BBC
Go toBBCAfrica.comfor more news from the African continent.
Focus on Africa
This Is Africa
Democratic Republic of Congo
Ebola virus
Africa
Disease
Viruses